
For many years, the question of whether mobile phone use increases the risk of brain tumors has carried significant weight in the broader debate over potential health risks from mobile phone radiation. Particular importance has been attached to the so-called Danish mobile phone cohort study — a study that has often been used as evidence that mobile phones do not cause cancer. However researchers show in a new article that the study in fact cannot say anything meaningful about the risk of brain tumors from mobile phone use. Moreover, its findings are contradicted by cancer statistics.
The Danish Cohort
The study was published in the British Medical Journal in 2011 under the title “Use of mobile phones and risk of brain tumours: update of Danish cohort study.”
It compared the incidence of brain tumors up to and including 2007 among more than 358,000 Danes who had at some point subscribed to a private mobile phone account between 1987 and 1995, with the incidence of brain tumors in a registry covering 3.21 million Danes aged 30 years or older. The latter group constituted a so-called control group, which was assumed to be unexposed. The researchers themselves described that they compared mobile phone subscribers and non-subscribers before 1995: “Participants: All Danes aged ≥30 and born in Denmark after 1925, subdivided into subscribers and non-subscribers of mobile phones before 1995.”
The study concluded that no increased risk of brain tumors was observed.
The Danish cohort study was initially funded in part by Danish telecom operators and an American consulting firm.
Numerous Systematic Errors
The critical review was conducted by researcher Lennart Hardell, former professor and senior physician at the Department of Oncology, Örebro University Hospital in Sweden, in collaboration with Mona Nilsson of the Swedish Radiation Protection Foundation. They primarily identify the following serious flaws in the Danish cohort study:
- The Danish cohort claims to compare brain tumor risk among early mobile phone users from 1987–1995 with 3.21 million people from the rest of the Danish population (aged 30 or older) who supposedly had no mobile subscriptions and were therefore assumed not to use mobile phones. However, more than 200,000 corporate subscription holders from 1982–1995 were excluded. They were instead placed in the control group — the rest of the population — which was supposed to be unexposed and which the researchers themselves described as a group without mobile subscriptions. These corporate users were, with high probability, by far the heaviest users, as shown by statistics on private and corporate users compiled by Hardell and Nilsson. Between 1999 and 2004, people with corporate subscriptions used mobile phones approximately five times more per month than private subscribers, according to official statistics from the Swedish Post and Telecom Authority (PTS). Thus, the most relevant group to study regarding brain tumor risks was excluded and instead included among those “who did not use mobile phones” or, as the researchers themselves described them, “non-subscribers.”
- In addition, more than 164,000 other subscription holders were excluded for other reasons.
- The unexposed control group — the rest of the population — became increasingly contaminated between 1995 and 2007 by new mobile phone subscribers. By 2005, Denmark had 100 subscriptions per 100 inhabitants.
- The Danish cohort completely lacked information on actual exposure, that is, whether and how much mobile phones were used among those classified as “users.” Instead, the researchers used the number of years since a person first signed up for a private mobile subscription during 1987–1995 as equivalent to years of “exposure” or “use” up to and including 2007.
- The study therefore had no possibility of comparing risk among exposed versus unexposed individuals, nor among the most highly exposed versus the least exposed.
Exposure unknown
A fundamental principle in epidemiological research is to compare exposed individuals with unexposed individuals and investigate whether the exposed group has an increased occurrence of the disease under study. Researchers may also divide exposed individuals into highly exposed and less exposed groups if no unexposed group exists, and then examine whether higher exposure leads to greater risk. This was never done by the researchers behind the Danish cohort study.
In the Danish cohort, exposure was based solely on the time elapsed since the first private subscription was signed and not on actual or self-reported mobile phone use.
Since the control group in practice increasingly consisted of mobile phone subscribers as well, the difference between the comparison groups became so small that the study was essentially meaningless with regard to risks associated with mobile phone use.
The Danish cohort study did not investigate whether mobile phone use — and especially not heavy use — leads to an increased risk of brain tumors compared with little or no use.
Danish Cohort Contradicted by Brain Tumor Statistics
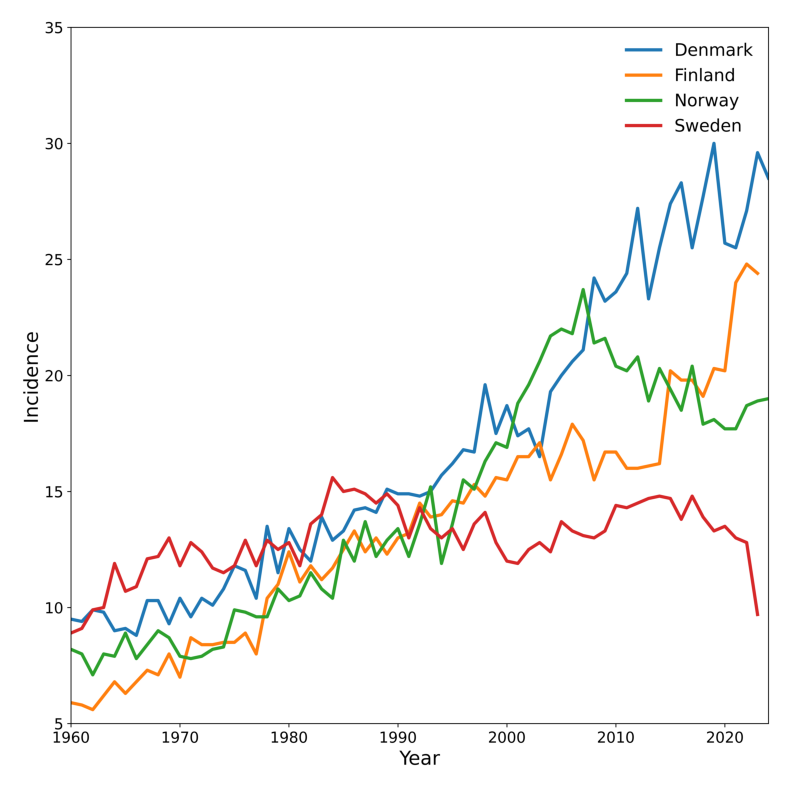
The authors of the cohort study have argued that their findings are supported by statistics from the Nordic countries’ cancer registries, which overall have not shown an increasing incidence of brain tumors. However, Hardell and Nilsson demonstrate in their critical analysis that the statistics from the individual Nordic countries differ substantially and that brain tumor incidence increased the most in Denmark. This directly contradicts the cohort study’s conclusions.
Hardell and Nilsson argue that the authors of the Danish cohort should have compared their results with Danish statistics specifically, rather than with aggregated Nordic data, which vary greatly between countries. The discrepancies are likely explained by differences in reporting practices to cancer registries.
It is therefore incorrect to categorically claim that brain tumors have not increased while mobile phone use has increased — some countries’ cancer statistics show increases, while others, such as Sweden’s, do not.
See the diagram below. Age standardized incidence (Nordic 2000) per 100 000 inhabitats per year 1960-2023 men and women combined in Denmark, Finland, Norway and Sweden.
Danish Cohort Given High Weight in WHO Evaluation
The new critical review also examined how the Danish cohort study has been assessed in several international and national expert evaluations. Most notably, the cancer risk evaluation commissioned by WHO and published in 2024 gave the Danish cohort study a high rating and substantial weight in the assessment of cancer risks from mobile phone use.
Several of the WHO evaluation authors are members of the organization ICNIRP, which established the exposure limits currently applied to radiation from mobile phones and recommended by organizations including WHO and the EU. These limits do not protect against cancer and are designed only to prevent heating effects. They would be invalidated if a cancer risk were officially recognized, with potentially enormous negative consequences for the mobile phone industry.
For example, the WHO evaluation gave the Danish cohort greater weight and a higher rating than both the large Interphone study published in 2010 and the findings of the Hardell group. The findings of Hardell and colleagues have been considered the most reliable by Italian courts. Both the Interphone study and the Hardell studies, in contrast to the Danish cohort, showed an increased risk of brain tumors among those who had used mobile phones the most in terms of total hours of use. Both studies investigated how much participants had actually used mobile phones.
These studies were a major reason why WHO’s International Agency for Research on Cancer (IARC) classified radiofrequency radiation from mobile phones in 2011 as “possibly carcinogenic to humans” (Group 2B).
References:
Lennart Hardell, Mona Nilsson: Exposure Misclassification in the Danish Mobile Phone Subscriber Cohort and its Influence on International Radiofrequency (RF) Radiation Cancer Risk Assessments. Archives of Internal Medicine Research. 9 (2026): 107-118. Link



